What is Contact Dermatitis?
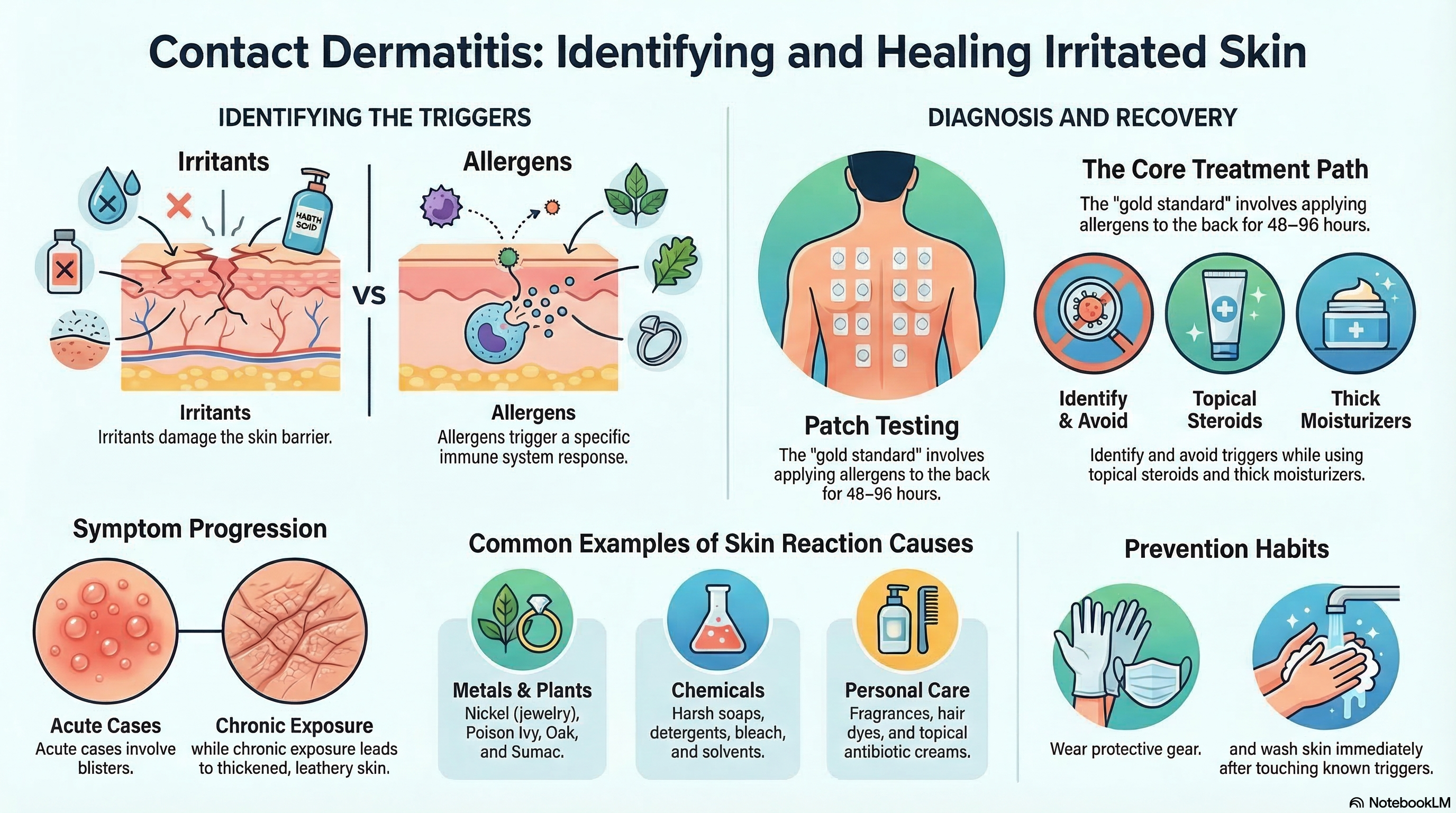
Contact dermatitis is categorized by how the skin appears and how long the reaction lasts. In the acute phase, you may see bright redness, swelling, and small, fluid-filled blisters that may ooze or "weep." If the exposure continues over a long period, it enters a chronic phase, where the skin becomes thickened, leathery (lichenified), and may develop painful cracks or fissures.
While it can appear anywhere, the hands are the most common site due to their frequent contact with chemicals, water, and tools. The location of the rash often provides a "clue" to the cause—for example, a rash on the earlobes often points to a nickel allergy from earrings, while a linear streak on the leg might suggest brushing against poison ivy.
Causes of Contact Dermatitis
The causes are divided based on whether the substance is an irritant or an allergen.
Common Irritants (Damage the skin barrier):
-
Chemicals: Harsh soaps, detergents, solvents, bleach, and acids.
-
Physical Factors: Frequent friction, extreme temperatures, or prolonged moisture (often seen in "diaper rash").
-
Occupational Materials: Cement, cutting oils, and fiberglass.
Common Allergens (Trigger an immune response):
-
Metals: Nickel (found in jewelry, belt buckles, and zippers) is the most common allergen worldwide.
-
Plants: Urushiol, the oil found in poison ivy, oak, and sumac.
-
Fragrances and Preservatives: Found in perfumes, cosmetics, wet wipes, and soaps (e.g., methylisothiazolinone).
-
Topical Medicines: Antibiotic creams like Neomycin or Bacitracin.
-
Personal Care Items: Hair dyes (PPD), nail polish, and latex/rubber found in gloves or elastic bands.
Symptoms of Contact Dermatitis
Symptoms typically stay confined to the area that touched the substance, though allergic reactions can sometimes spread slightly beyond the original site.
-
Redness and Swelling: The skin looks inflamed and may feel warm.
-
Itching (Pruritus): This is the hallmark of allergic reactions and can be intense.
-
Burning or Stinging: More common with irritants, often felt immediately or shortly after contact.
-
Blisters: Small (vesicles) or large (bullae) fluid-filled bumps that may crust over.
-
Dryness and Cracking: In chronic cases, the skin may become very dry, scaly, and develop deep, painful cracks.
Diagnosis of Contact Dermatitis
To treat the rash effectively, your doctor must determine exactly what caused it.
-
Exposure History: Your doctor will ask detailed questions about your job, hobbies, skincare routine, and any new products you’ve used.
-
Physical Exam: The pattern and location of the rash are critical. A rash around the waistband suggests a metal allergy from a button, while a rash on the face may suggest a cosmetic or airborne trigger.
-
Patch Testing (Gold Standard for Allergies): If an allergy is suspected, a dermatologist will perform a patch test. Small amounts of various allergens are applied to patches on your back and left for 48 hours. The skin is then checked at 48 hours and again at 96 hours to see which substances caused a localized reaction.
-
Note: This is different from a "scratch test" used for hay fever or food allergies.
-
Treatment of Contact Dermatitis
The most important step in treatment is identifying and avoiding the trigger. If you continue to touch the substance, the rash will likely return or never fully heal.
-
Topical Steroids: These are the mainstay of treatment to reduce inflammation. Your doctor may prescribe a mild cream for the face or a high-potency ointment for thickened skin on the hands or feet.
-
Skin Barrier Restoration: Frequently applying thick, fragrance-free moisturizers or petroleum jelly helps repair the damaged skin barrier.
-
Cool Compresses: Applying a cool, damp cloth can soothe itching and help dry out weeping blisters.
-
Systemic Treatment: For severe cases (like a widespread poison ivy rash), your doctor may prescribe oral corticosteroids (prednisone). These are usually tapered over 2–3 weeks to prevent the rash from rebounding.
-
Non-Steroid Creams: For sensitive areas like the eyelids or face, "calcineurin inhibitors" (like tacrolimus) may be used to avoid the side effects of long-term steroid use.
Prevention of Contact Dermatitis
Preventing future flare-ups requires a proactive approach to skin protection.
-
Identify Your Triggers: Once a patch test identifies an allergen, read labels carefully. Many chemicals go by multiple names.
-
Use Protective Gear: Wear gloves when handling cleaning supplies or chemicals. Ensure the glove material itself (like rubber or latex) isn't something you are allergic to.
-
Wash Skin Promptly: If you know you’ve touched an irritant or allergen (like poison ivy), wash the area immediately with mild soap and water to remove the substance before it penetrates the skin.
-
Apply Barrier Creams: Creams containing dimethicone can provide an extra layer of protection for people whose jobs involve frequent contact with water or mild irritants.
-
Choose Fragrance-Free: Switch to "hypoallergenic" or fragrance-free soaps and moisturizers to minimize the risk of sensitization.