What is Constipation?
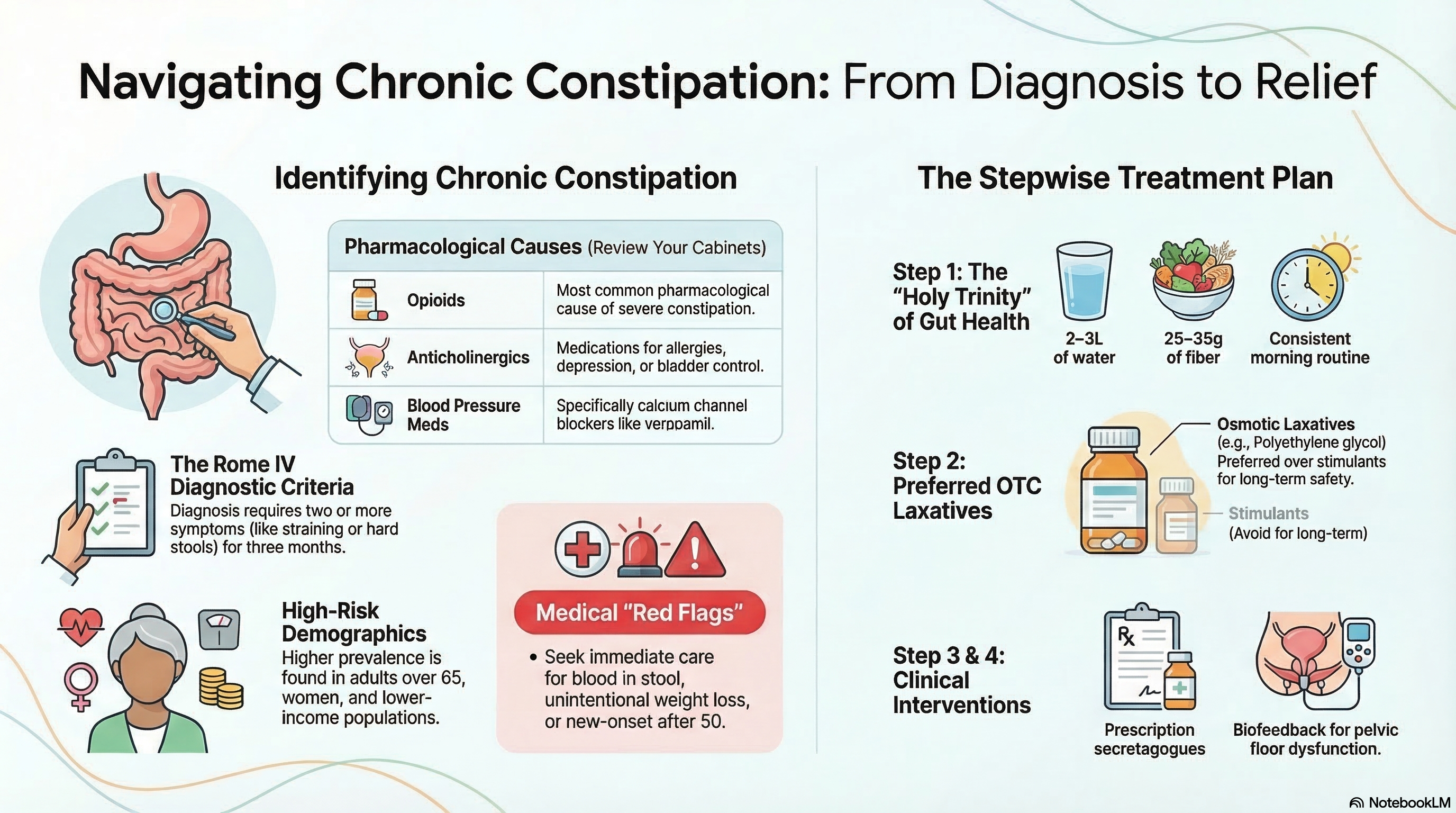
While "normal" bowel frequency ranges from three times a day to three times a week, doctors use specific criteria (the Rome IV criteria) to diagnose chronic constipation. You may be diagnosed with chronic constipation if you have experienced at least two of the following symptoms for at least three months:
-
Fewer than three spontaneous bowel movements per week.
-
Straining during more than 25% of bowel movements.
-
Lumpy or hard stools (Type 1 or 2 on the Bristol Stool Scale).
-
A sensation of incomplete evacuation (feeling like you didn't "finish").
-
A sensation of a blockage in the anorectal area.
-
The need for manual maneuvers (using fingers) to help pass stool.
Constipation is generally categorized into two types: Primary (Functional), which is a problem with how the colon or pelvic muscles move, and Secondary, which is caused by an underlying disease or medication.
Causes of Constipation
Constipation can be caused by lifestyle habits, medical conditions, or side effects from medications.
Lifestyle and Diet
-
Low Fiber: Not eating enough fruits, vegetables, and whole grains.
-
Dehydration: Inadequate fluid intake makes stool harder and more difficult to pass.
-
Inactivity: A sedentary lifestyle slows down the natural contractions of the intestines.
-
Ignoring the Urge: Repeatedly delaying a bowel movement can lead to the loss of the "urge" over time.
Medical Conditions
-
Metabolic: Hypothyroidism, diabetes, or high calcium levels (hypercalcemia).
-
Neurological: Parkinson’s disease, multiple sclerosis, or spinal cord injuries.
-
Pelvic Floor Dysfunction: Lack of coordination in the muscles used during a bowel movement.
Medications (The "Top Offenders")
-
Opioids: These are the most common pharmacological cause of severe constipation.
-
Anticholinergics: Used for allergies, depression (amitriptyline), or bladder control.
-
Blood Pressure Meds: Specifically calcium channel blockers like verapamil.
-
Supplements: Iron and calcium supplements are frequent causes of hardened stools.
Demographics and Risk Factors Statistics show that certain groups are more likely to experience constipation:
-
Age: Adults over 65 are at higher risk due to slowed motility and increased medication use.
-
Gender: It is more common in women, particularly during pregnancy or after menopause.
-
Race: Higher prevalence is noted among non-White individuals.
-
Socioeconomic Status: Lower income levels correlate with higher rates, often due to limited access to high-fiber foods or exercise opportunities.
Symptoms of Constipation
Beyond the "Core Symptoms" used for diagnosis, constipation can cause several secondary physical issues:
-
Abdominal Bloating and Gas: Discomfort or a "heavy" feeling in the stomach.
-
Abdominal Pain: Cramping that is often relieved after a bowel movement.
-
Hemorrhoids or Anal Fissures: Caused by persistent straining and passing hard stools.
Red Flags (Seek Medical Attention Immediately): You should see a doctor urgently if you experience:
-
New-onset constipation after age 50.
-
Blood in your stool (bright red or black/tarry).
-
Unintentional weight loss.
-
Severe abdominal pain or vomiting.
-
Iron-deficiency anemia.
Diagnosis of Constipation
Most cases of constipation are diagnosed through a detailed medical history and a physical exam.
-
Initial Evaluation: Your doctor will review your medications and may perform a digital rectal exam to check for blockages or muscle coordination.
-
Laboratory Tests: Routine blood work is generally not needed unless the doctor suspects a secondary cause like hypothyroidism or high calcium.
-
Colonoscopy: This is only recommended if you have "red flag" symptoms or are due for your routine colorectal cancer screening.
-
Specialized Testing: If you do not respond to initial treatment, your doctor may order:
-
Anorectal Manometry: To check how the muscles in your rectum and anus work together.
-
Transit Studies: Using a "wireless motility capsule" or markers to see how fast food moves through your colon.
-
Treatment of Constipation
Doctors recommend a stepwise approach, starting with the simplest lifestyle changes before moving to medications.
Step 1: Lifestyle and Fiber
-
Fiber: Gradually increase soluble fiber (psyllium, oats, beans) to a goal of 25–35 grams per day.
-
Fluid: Aim for 2–3 liters of water daily to support the increased fiber.
-
Routine: Set aside 10 minutes after breakfast to sit on the toilet without distractions.
Step 2: Over-the-Counter (OTC) Laxatives
-
Osmotic Laxatives (Preferred): Polyethylene glycol (MiraLAX) is the safest and most effective option for long-term use. It works by pulling water into the colon to soften the stool.
-
Stimulant Laxatives: Medications like Senna or Bisacodyl can be used occasionally but should not be the first choice for daily use.
Step 3: Prescription Medications If OTC options fail, your doctor may prescribe "secretagogues" like linaclotide (Linzess) or lubiprostone (Amitiza), which increase fluid secretion in the gut. For opioid-induced constipation, specific "mu-opioid receptor antagonists" (like naloxegol) may be required.
Step 4: Advanced Therapies
-
Biofeedback: This is the gold-standard treatment for pelvic floor dysfunction (dyssynergic defecation), with a 70–80% success rate. It teaches you how to coordinate your muscles during defecation.
-
Surgery: A colectomy is a rare, last-resort option only for patients with severe "slow-transit" constipation that has failed all other treatments.
Prevention of Constipation
The best way to manage constipation is to prevent it from becoming a chronic issue.
-
Maintain the "Holy Trinity" of Gut Health: High fiber, high fluid intake, and regular daily exercise (like a 30-minute walk).
-
Listen to Your Body: When you feel the urge to go, go. Delaying it makes the stool harder and more difficult to pass later.
-
Review Your Meds: If you are starting a new medication known to cause constipation (like an opioid), talk to your doctor about starting a "bowel regimen" at the same time.
-
Positioning: Using a small footstool to elevate your knees while on the toilet can help straighten the anorectal angle, making it easier for stool to pass.