What is Compartment Syndrome?
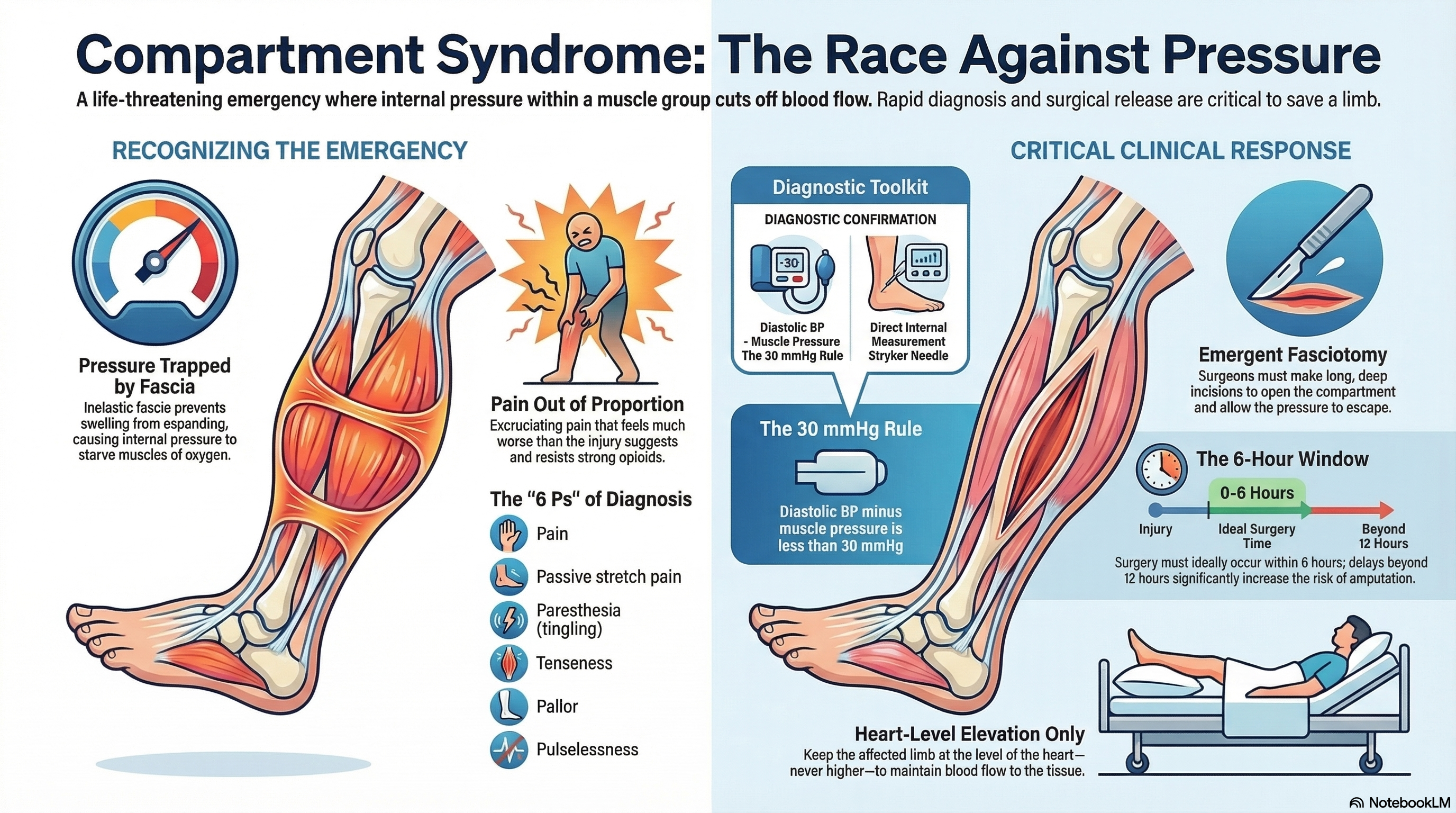
Compartment syndrome is a surgical emergency that occurs when excessive pressure builds up within a closed muscle "compartment." In the human body, muscles, nerves, and blood vessels are grouped together in areas surrounded by a tough, inelastic web of tissue called fascia. Because the fascia does not stretch, any swelling or bleeding within that space causes the internal pressure to rise rapidly.
This high pressure restricts blood flow to the affected area, starving muscles and nerves of oxygen (ischemia). If the pressure is not released quickly, it can lead to permanent muscle death, nerve damage, or even the loss of a limb. While it most commonly affects the lower leg and the forearm, it can occur in the hand, foot, thigh, or upper arm.
Causes of Compartment Syndrome
There are two distinct types of this condition, each triggered by different circumstances:
Acute Compartment Syndrome (ACS) This is a life-threatening emergency usually caused by a sudden, severe injury. Common triggers include:
-
Fractures: Roughly 40% of cases are caused by broken bones, particularly in the lower leg (tibia) or forearm.
-
Crush Injuries: Massive pressure on a limb, even without a broken bone.
-
Tight Wrappings: Constricting bandages, casts, or even circumferential burns that act like a vice on the limb.
-
Vascular Issues: Bleeding disorders or a "reflux" of blood flow after a blocked artery has been repaired.
-
Other Triggers: Snake bites, severe bruising, or even intense intravenous fluid infusions.
Chronic Exertional Compartment Syndrome (CECS) This is a non-emergency condition typically seen in young athletes, such as runners or soccer players. It is caused by repetitive, high-impact exercise that causes the muscles to expand temporarily, increasing pressure only during the workout.
Symptoms of Compartment Syndrome
Recognizing the symptoms early is the most critical step in saving a limb. Doctors look for the "6 Ps," though the first two are the most reliable indicators.
-
Pain Out of Proportion: This is the hallmark sign. The pain feels much more severe than the injury should suggest and is not relieved by strong pain medications (opioids).
-
Pain with Passive Stretch: If a doctor gently moves your fingers or toes to stretch the affected muscle, it causes excruciating pain.
-
Paresthesia: A "pins and needles" sensation, tingling, or numbness in the limb.
-
Palpably Tense: The area feels rock-hard to the touch, often compared to the tension of a drum.
-
Pallor and Pulselessness: These are very late signs indicating the blood flow has almost entirely stopped. Waiting for these symptoms to appear can be dangerous.
In children, look for the "Three As": Agitation, Anxiety, and an increasing need for Analgesics (pain medicine).
Diagnosis of Compartment Syndrome
A diagnosis is primarily made through a physical examination and a high degree of suspicion following an injury.
-
Clinical Assessment: In an awake patient, a doctor can usually diagnose the condition based on the severity of the pain and the "hardness" of the compartment.
-
Pressure Measurement: If a patient is unconscious or the diagnosis is unclear, a doctor may use a specialized needle (Stryker needle) attached to a monitor to measure the exact pressure inside the muscle.
-
The 30 mmHg Rule: If the difference between your diastolic blood pressure and the pressure inside your muscle is less than 30 mmHg, it confirms that the blood can no longer flow properly into the tissue.
Treatment of Compartment Syndrome
For Acute Compartment Syndrome, there is only one definitive treatment: Emergent Fasciotomy.
-
The Procedure: A surgeon makes long, deep incisions through the skin and the fascia to "open" the compartment and allow the pressure to escape.
-
Wound Care: These incisions are left open (not stitched) to ensure the pressure does not return as the swelling goes down. They are usually closed several days later with a skin graft or stitches.
-
Timing: For the best results, surgery should happen within 6 hours of the onset of symptoms. Delays beyond 12 hours significantly increase the risk of permanent disability or amputation.
For Chronic (Exertional) Compartment Syndrome, treatment is usually elective. It may involve physical therapy, changing your exercise routine, or a scheduled, less-invasive version of the fasciotomy if the pain prevents you from participating in sports.
Prevention of Compartment Syndrome
While you cannot always prevent a traumatic injury, you can take steps to reduce the risk of the pressure becoming dangerous.
-
Cast Safety: If you have a cast or a tight bandage, inform your doctor immediately if you feel increasing pain, numbness, or if your fingers/toes turn blue or cold.
-
Elevation with Caution: While elevation is usually good for swelling, in a suspected case of compartment syndrome, the limb should be kept at the level of the heart—not higher—to ensure blood can still reach the area.
-
Monitoring High-Risk Fractures: If you have a tibia or forearm fracture, your medical team will monitor you closely for the first 24 to 48 hours, as this is when the pressure is most likely to spike.
-
Chronic Management: For athletes, gradual training and proper footwear can help manage exertional pressure. If you feel a burning or aching pain that starts and stops at a specific point in your workout, seek a sports medicine evaluation early.