What is Cluster Headache?
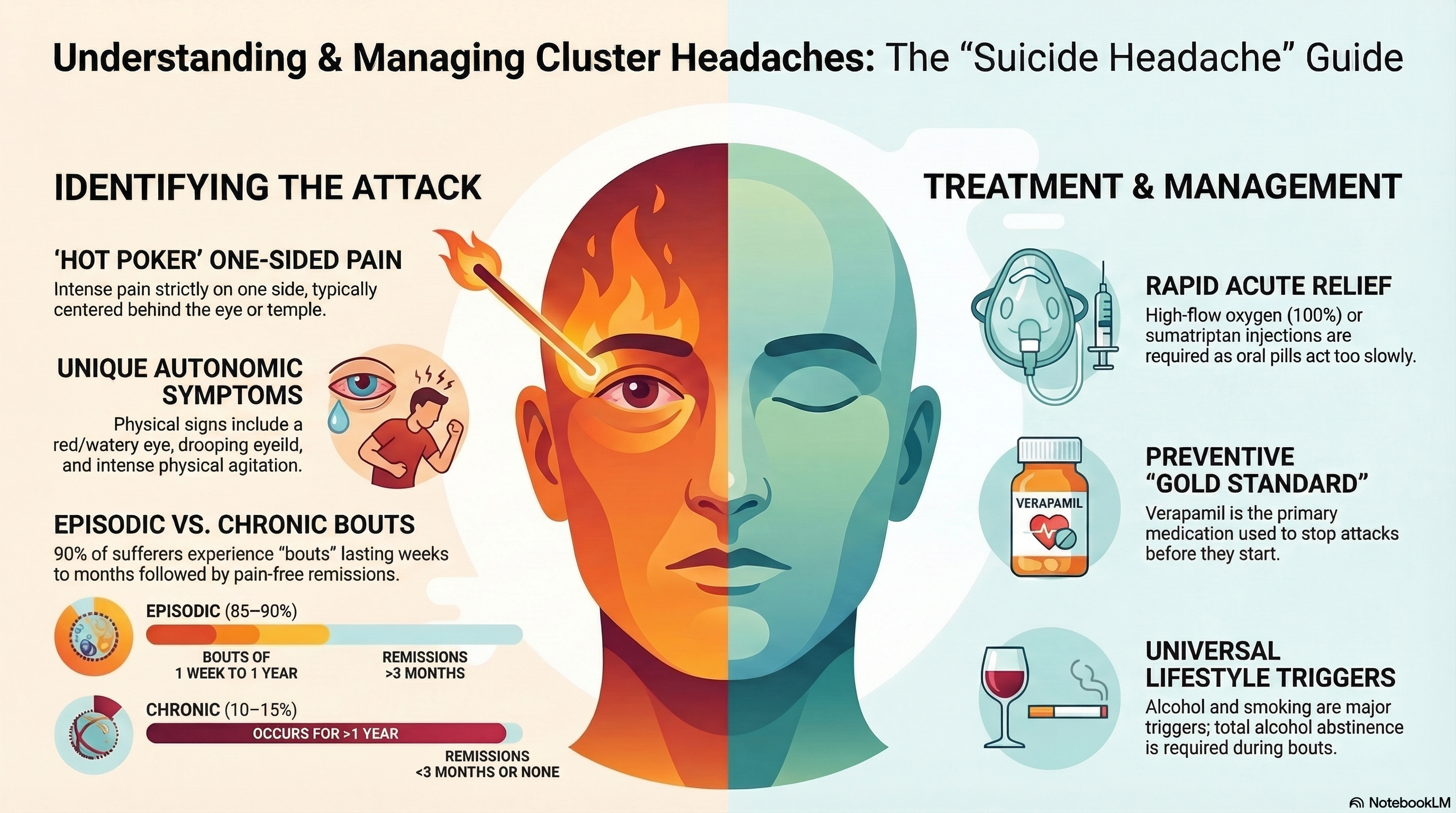
A cluster headache is characterized by sudden, excruciatingly painful attacks that are strictly one-sided. The pain is usually felt around or behind one eye, the temple, or the upper face. Patients often describe the sensation as a "hot poker in the eye" or like the eye is being "pulled out."
The disorder is classified into two main types:
-
Episodic Cluster Headache (85–90%): Attacks occur in "bouts" or cluster periods lasting from one week to a year, followed by pain-free remission periods of at least three months.
-
Chronic Cluster Headache (10–15%): Attacks occur for more than a year without a remission period, or with remissions that last less than three months.
Causes of Cluster Headache
While the exact cause is not fully understood, research suggests that the condition is linked to a sudden release of histamine or serotonin in the area of the trigeminal nerve, the main nerve responsible for sensation in the face.
Key Factors and Triggers:
-
The Hypothalamus: The extreme regularity of attacks (often occurring at the same time every night) suggests an abnormality in the hypothalamus, the part of the brain that regulates the body's internal clock.
-
Genetics: First-degree relatives of sufferers have a 5 to 18 times higher risk of developing the condition.
-
Lifestyle: There is a strong association with heavy smoking; 70% to 90% of patients are current or former smokers.
-
Reliable Triggers: During a cluster period, alcohol is a near-universal trigger. Other triggers include strong smells (petrol, paint, or perfume), heat, and napping during the day.
Symptoms of Cluster Headache
An attack usually begins suddenly and lasts between 15 and 180 minutes. The pain is almost always unilateral, meaning it stays on the same side of the head throughout the entire cluster period.
Autonomic Symptoms (occurring on the same side as the pain):
-
A red, watering eye (conjunctival injection and lacrimation).
-
A drooping or swollen eyelid (ptosis).
-
A constricted or dilated pupil.
-
Nasal congestion or a runny nose.
-
Facial sweating.
A hallmark behavioral symptom is agitation. Unlike other headaches, patients feel a desperate need to move and cannot lie still.
Diagnosis of Cluster Headache
Diagnosis is based entirely on the clinical history provided by the patient. Because cluster headaches are rare, they are frequently misdiagnosed as migraines or sinus infections.
-
Clinical Criteria: Doctors look for the specific duration (15–180 minutes), the frequency (up to 8 times daily), and the presence of the autonomic symptoms mentioned above.
-
Neuroimaging: While a CT scan or MRI cannot "see" a cluster headache, imaging is usually performed at least once to rule out secondary causes or structural abnormalities in the brain.
-
Symptom Tracking: Keeping a detailed headache diary that tracks the timing, duration, and triggers of your attacks is the most helpful tool for your specialist.
Treatment of Cluster Headache
Because the pain is so rapid and severe, oral tablets are generally ineffective because they take too long to absorb. Treatment is divided into acute relief and long-term prevention.
Acute (Abortive) Treatment:
-
High-Flow Oxygen: Inhaling 100% oxygen at 12–15 liters per minute through a non-rebreather mask can stop an attack in 10–15 minutes for 70–80% of patients.
-
Subcutaneous Sumatriptan: An injection of 6 mg is the fastest pharmacological option, providing relief for most patients within 15 minutes. Nasal sprays (Zolmitriptan) are also used but may be slightly less effective.
Preventive and Transitional Treatment:
-
Verapamil: The gold standard for prevention. It requires ECG monitoring as it can affect heart rhythm.
-
Galcanezumab (Emgality): An FDA-approved monthly injection specifically for preventing episodic cluster headaches.
-
Bridge Therapy: While waiting for preventives to kick in, doctors may use a Prednisone (steroid) taper or occipital nerve blocks to suppress attacks temporarily.
-
Neuromodulation: Devices that stimulate the vagus nerve (gammaCore) or the sphenopalatine ganglion (SPG) can be used as non-drug alternatives.
Prevention of Cluster Headache
Preventing cluster headaches involves both medication and strict lifestyle modifications during a cluster period.
-
Alcohol Abstinence: During a cluster bout, you must avoid alcohol entirely, as it acts as a nearly immediate trigger for an attack.
-
Smoking Cessation: Quitting smoking has been shown to improve the long-term prognosis and may lead to longer remission periods.
-
Regular Sleep Schedule: Since attacks are linked to the body's internal clock, maintaining a consistent sleep routine and avoiding afternoon naps can help reduce the frequency of "hypnic" (sleep-waking) attacks.
-
Trigger Avoidance: Avoid exposure to strong chemical smells, solvents, and excessive heat during your active periods.