What is Atopic Dermatitis?
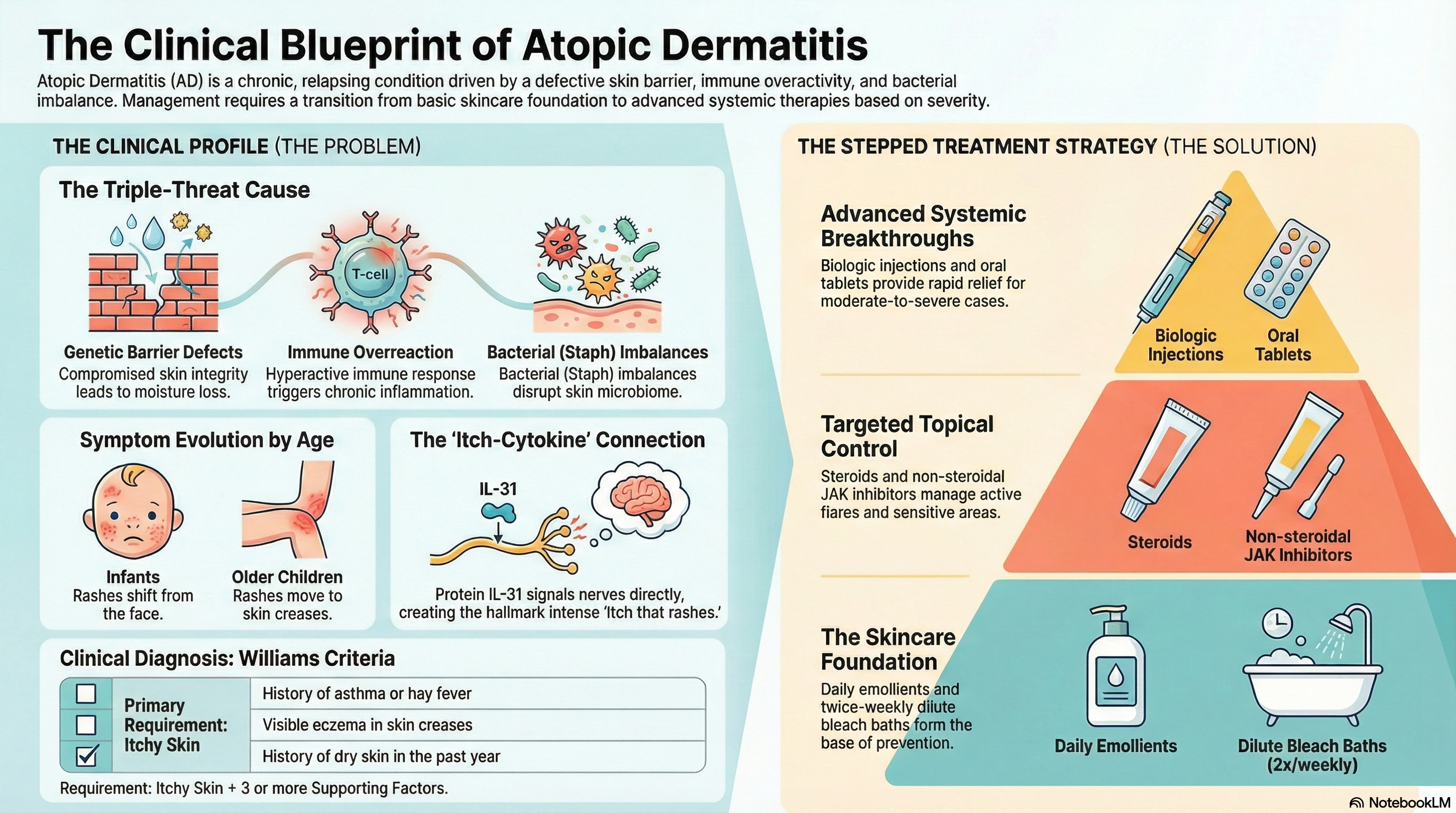
Atopic dermatitis is characterized by a "relapsing" course, meaning symptoms go through periods of "flares" (worsening) and remissions (clearing). It is defined by a triad of features: a defective skin barrier, an overactive immune system, and an imbalance in the skin's natural bacteria.
The condition varies significantly based on age:
-
Infants (0–2 years): Rashes typically appear on the face, scalp, and the outer sides of the arms and legs. Interestingly, the diaper area is usually spared.
-
Children (2–12 years): The rash often moves to the "flexural" areas—the creases of the elbows and the backs of the knees—as well as the wrists and ankles.
-
Adults: Skin often becomes thick, leathery, and hyperpigmented (lichenification) due to years of scratching, commonly affecting the hands, eyelids, and neck.
Causes of Atopic Dermatitis
The cause of atopic dermatitis is a combination of genetics, your environment, and your immune system.
Genetic Factors The most significant genetic factor is a mutation in the filaggrin (FLG) gene, which affects 30–50% of White patients. Filaggrin is a protein that helps build the "bricks and mortar" of the skin barrier. Without it, moisture escapes (dryness) and irritants/allergens can easily enter the skin.
Immune Dysregulation In people with this condition, the immune system overreacts to minor triggers. Specifically, proteins called interleukins (IL-4, IL-13, and IL-31) drive the inflammation. IL-31 is known as the "itch cytokine" because it directly signals your nerves to feel itchy.
Environmental Triggers
-
Climate: Cold weather and low humidity can dry out the skin.
-
Irritants: Harsh soaps, detergents, fragrances, and wool clothing.
-
Microbes: Over 90% of patients have Staphylococcus aureus bacteria on their skin, which can worsen inflammation.
-
The Hygiene Hypothesis: Living in urban, highly sanitized environments may prevent the immune system from "learning" correctly in early childhood, increasing the risk of eczema.
Symptoms of Atopic Dermatitis
The hallmark of atopic dermatitis is pruritus—an itch so intense that it is often described as "the itch that rashes."
-
Intense Itching: Often worse at night, leading to significant sleep loss.
-
Dry, Scaly Skin: A general dryness known as xerosis.
-
Red to Brownish-Gray Patches: These can appear anywhere but are most common in skin folds.
-
Small, Raised Bumps: These may leak fluid and "weep" when scratched.
-
Lichenification: Thickened, leathery skin caused by repeated scratching.
-
Associated Signs: You may notice "Dennie-Morgan folds" (extra creases under the eyes) or "keratosis pilaris" (small, rough bumps on the upper arms and thighs).
Diagnosis of Atopic Dermatitis
Atopic dermatitis is a "clinical diagnosis," meaning there is no single blood test or skin biopsy that can confirm it. Instead, doctors use specific criteria based on your history and physical appearance.
Diagnostic Criteria Doctors often look for the "Williams Criteria," which requires itchy skin plus three or more of the following:
-
A history of skin crease involvement (elbows, knees, ankles).
-
A personal history of asthma or hay fever.
-
A history of generally dry skin in the past year.
-
Visible eczema in the creases.
-
Symptoms beginning before the age of two.
Supporting Tests While not diagnostic, a doctor may check Serum IgE levels (elevated in 80% of cases) or perform a skin swab if they suspect a bacterial or viral infection like "eczema herpeticum"—a medical emergency caused by the cold sore virus.
Treatment of Atopic Dermatitis
Treatment follows a "stepped" approach, moving from basic skin care to advanced therapies depending on severity.
The Foundation: Skin Care
-
Emollients: These are thick, fragrance-free moisturizers (ointments are better than creams). They should be applied at least twice daily and within three minutes of bathing to "lock in" moisture.
-
Bleach Baths: Dilute bleach baths (1/2 cup for a full tub) twice a week can reduce the bacteria on the skin and decrease the frequency of flares.
Topical Medications
-
Corticosteroids (TCS): The mainstay for treating flares. They range from mild (hydrocortisone) to super-potent.
-
Calcineurin Inhibitors: Non-steroidal creams like Tacrolimus or Pimecrolimus, safe for sensitive areas like the face and eyelids.
-
JAK Inhibitors: Newer creams like Ruxolitinib that target the internal signaling of the itch-scratch cycle.
Advanced Systemic Therapies For moderate-to-severe cases, doctors may prescribe:
-
Biologics: Injections like Dupilumab or Tralokinumab that block the specific interleukins causing the inflammation. These are highly effective and do not require regular blood monitoring.
-
Oral JAK Inhibitors: Daily tablets (like Upadacitinib) that provide very rapid relief from itching, often within days.
-
Phototherapy: Controlled exposure to narrowband UVB light.
Prevention of Atopic Dermatitis
While you cannot change your genetics, you can take steps to prevent flares and potentially stop the "atopic march."
Managing the Barrier The most effective way to prevent flares is "proactive therapy." This involves using your prescribed medicated creams twice a week on "hot spot" areas even when the skin looks clear. This keeps the inflammation under the surface from erupting.
Environmental Control
-
Cotton Clothing: Avoid wool and scratchy synthetics.
-
Lukewarm Showers: Limit bathing to 10–15 minutes in lukewarm (not hot) water.
-
Trigger Identification: Keep a diary to see if certain foods, pets, or detergents coincide with your flares.
Early Intervention in Infants There is mixed evidence regarding "primary prevention." Some studies suggest that applying emollients daily from birth in high-risk infants (those with a parent or sibling with eczema) may reduce the risk of the child developing the condition, though recent large-scale trials have been less conclusive.