What is Ankylosing Spondylitis?
Ankylosing spondylitis (AS) is a chronic, progressive form of autoimmune inflammatory arthritis that primarily targets the spine and the sacroiliac joints, where the base of the spine meets the pelvis. It is the prototype of a group of diseases known as axial spondyloarthritis.
The word "ankylosing" means stiffening or fusing, while "spondylitis" refers to inflammation of the vertebrae. If left untreated, the chronic inflammation can cause the body to produce extra calcium around the segments of the spine, eventually leading to permanent fusion. This can result in a "bamboo spine" appearance on X-rays, significantly reducing spinal flexibility and increasing the risk of fractures. AS typically begins between the ages of 15 and 40 and affects approximately 0.1% to 1.4% of the population. While traditionally thought to be more common in men, it is now understood that women are frequently underdiagnosed because they often present with more peripheral joint pain rather than classic spinal fusion.
Causes of Ankylosing Spondylitis
The exact cause of AS is not fully understood, but it is driven by a complex interaction between genetics and the immune system.
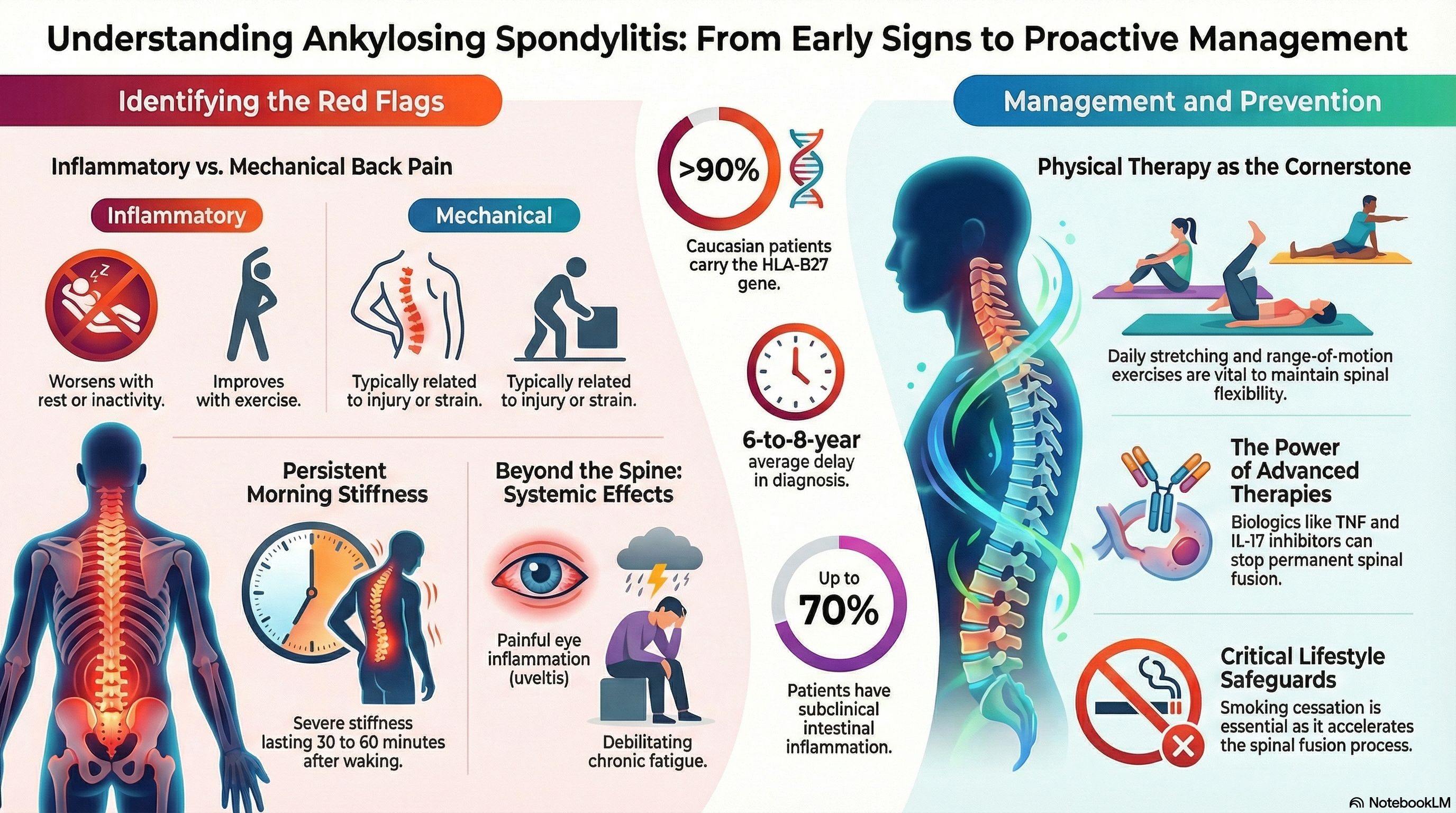
Genetic Predisposition The strongest risk factor is the HLA-B27 gene. More than 90% of Caucasian patients with AS carry this gene marker. However, it is important to note that carrying the gene does not guarantee you will develop the disease; many people have the gene but never experience symptoms.
Immune System and Gut Health Recent research suggests that "gut microbial dysbiosis" (an imbalance of bacteria in the digestive tract) may play a role. Up to 70% of patients have subclinical intestinal inflammation. It is believed that certain triggers may cause the immune system to attack the "entheses"—the specific points where tendons and ligaments attach to the bone.
Demographics and Risk
-
Ethnicity: Prevalence is higher in people of Northern European descent.
-
Family History: Having a first-degree relative with AS significantly increases your risk.
-
Age: Onset is rare after age 45.
Symptoms of Ankylosing Spondylitis
The hallmark of AS is "inflammatory back pain," which differs significantly from the mechanical back pain most people experience from injury or strain.
Spinal and Joint Symptoms
-
Gradual Onset: Pain that develops slowly over months rather than after a specific injury.
-
Morning Stiffness: Severe stiffness lasting 30 to 60 minutes or longer upon waking.
-
Improvement with Movement: Unlike a pulled muscle, AS pain feels better with exercise and worse with rest or inactivity.
-
Nocturnal Pain: Pain that often wakes you up in the second half of the night.
-
Enthesitis: Tenderness at the heels (Achilles tendon), chest wall, or hips.
Extra-articular Symptoms (Outside the Joints) AS is a systemic disease, meaning it can affect other parts of the body:
-
Uveitis: A painful, red "hot" eye with light sensitivity. This affects 30–40% of patients.
-
Fatigue: A deep, debilitating exhaustion caused by the body's constant state of inflammation.
-
Psoriasis: Skin rashes associated with inflammation.
-
IBD: Chronic digestive issues like Crohn's disease or Ulcerative Colitis.
Diagnosis of Ankylosing Spondylitis
Diagnosis is often delayed by an average of 6 to 8 years because early symptoms can mimic common back pain. There is no single test for AS; instead, rheumatologists use a combination of clinical history, blood work, and imaging.
Imaging Stages
-
MRI: This is the gold standard for early diagnosis (the "non-radiographic" stage). It can detect "bone marrow edema" or active inflammation before any permanent damage is visible on an X-ray.
-
X-ray: Used to look for structural changes or "radiographic" sacroiliitis. Once the spine shows fusion or "squaring" of the vertebrae, the disease is considered classic AS.
Laboratory Findings
-
HLA-B27 Testing: A blood test to check for the genetic marker.
-
Inflammatory Markers: Tests for C-reactive protein (CRP) and Erythrocyte Sedimentation Rate (ESR). While elevated in many, these markers are actually normal in about 30–50% of people with active disease.
Treatment of Ankylosing Spondylitis
While there is currently no cure, modern treatments have transformed the prognosis for AS. The goals are to reduce pain, maintain a straight posture, and prevent permanent spinal fusion.
Physical Therapy and Exercise This is the cornerstone of treatment. Daily stretching and range-of-motion exercises are vital to keep the spine flexible. Formal physical therapy helps patients maintain their posture and chest expansion.
First-Line Medication NSAIDs (Nonsteroidal Anti-inflammatory Drugs) such as naproxen, indomethacin, or celecoxib are the first choice. About 70% of patients respond well, though they often require high, consistent doses to manage the inflammation.
Second-Line: Biologics and JAK Inhibitors If NSAIDs are not enough, "Advanced Therapies" are used to block specific proteins in the immune system:
-
TNF Inhibitors: Injectable medications (like adalimumab or etanercept) that have a high success rate in reducing spinal symptoms.
-
IL-17 Inhibitors: Effective for those who also have psoriasis or those who do not respond to TNF blockers.
-
JAK Inhibitors: A newer class of oral tablets (like upadacitinib) that provide a highly effective non-injectable option.
Prevention of Ankylosing Spondylitis
Because AS is a genetic autoimmune condition, it cannot be prevented in the traditional sense. However, you can "prevent" the progression of the disease and its most severe complications.
Early Intervention The most effective way to prevent spinal fusion is early diagnosis and the prompt start of biologic therapy. Starting these treatments during the "non-radiographic" stage—before damage appears on X-rays—offers the best chance of maintaining a full range of motion.
Lifestyle and Safety
-
Smoking Cessation: Smoking is highly detrimental for AS patients. It increases spinal inflammation and accelerates the fusion process.
-
Posture Awareness: Sleeping on a firm mattress with a thin pillow (or no pillow) can help prevent the spine from fusing in a forward-leaning position.
-
Injury Prevention: Because a fused spine is brittle, even minor falls can cause serious fractures. Maintaining core strength and balance is essential for safety.
-
Cardiovascular Health: Chronic inflammation increases the risk of heart disease, so managing blood pressure and cholesterol is a key part of long-term prevention.